

Summarize this documentation using AI
GLP-1 patient retention is the discipline of keeping a patient on therapy long enough to reach a clinically meaningful outcome — through onboarding, adherence nudges, refill orchestration, and side-effect support — rather than letting them churn in the first weeks. It matters because the single biggest threat to a GLP-1 brand is not acquisition cost. It is that most patients stop before the medication has a chance to work. Blue Health Intelligence, analyzing nearly 170,000 commercial members, found 58% of patients discontinue before reaching a clinically meaningful health benefit, with 30% stopping within the first month and roughly 80% off the drug by 12 months. For a subscription telehealth model, that is a retention emergency disguised as a fulfillment problem.
Key Takeaways
- The drop-off is front-loaded. Blue Health Intelligence reports 30% of GLP-1 patients quit in month one — the same window where onboarding and side-effect coaching have the most leverage.
- Six-month discontinuation runs ~30%+ even in obesity cohorts. A JAMA-published analysis found 26.2% discontinued at 3 months and 30.8% at 6 months.
- Two-year persistence collapses. A widely cited study found 85% of weight-loss GLP-1 patients discontinue within two years.
- The market is enormous and getting more competitive. The GLP-1 receptor agonist market is roughly $82B in 2026 growing at ~12.4% CAGR — meaning retention, not access, becomes the moat.
- Retention is a lifecycle system, not a discount. The fix is onboarding that sets the first 30 days up as the product, side-effect anticipation, and refill orchestration — the same architecture that powers DTC telemedicine retention.
What GLP-1 Patient Retention Actually Means
In a DTC telehealth context, a GLP-1 patient is not a one-time buyer — they are a subscriber to an outcome. Retention means the percentage of patients who stay on therapy (and on your platform) across consecutive refill cycles until they reach the clinical result they signed up for. This is different from a standard DTC retention funnel in one crucial way: the product only works if the patient stays compliant, and compliance is fragile in the first weeks because of nausea, injection anxiety, cost shock, and unrealistic timeline expectations. A retained GLP-1 patient is a clinical win and a commercial one; a churned patient is usually a patient who never got the support they needed, not one who "didn't want it."
That reframing is the whole game. When brands treat discontinuation as inevitable, they over-invest in acquisition to refill a leaking bucket. When they treat it as a solvable lifecycle problem, they build the compounding LTV that makes the unit economics work. Propel's teardown of how Hims & Hers rebuilt retention around GLP-1 shows what happens when a brand treats the therapy journey — not the checkout — as the product.
Why Patients Quit — The Four Real Reasons
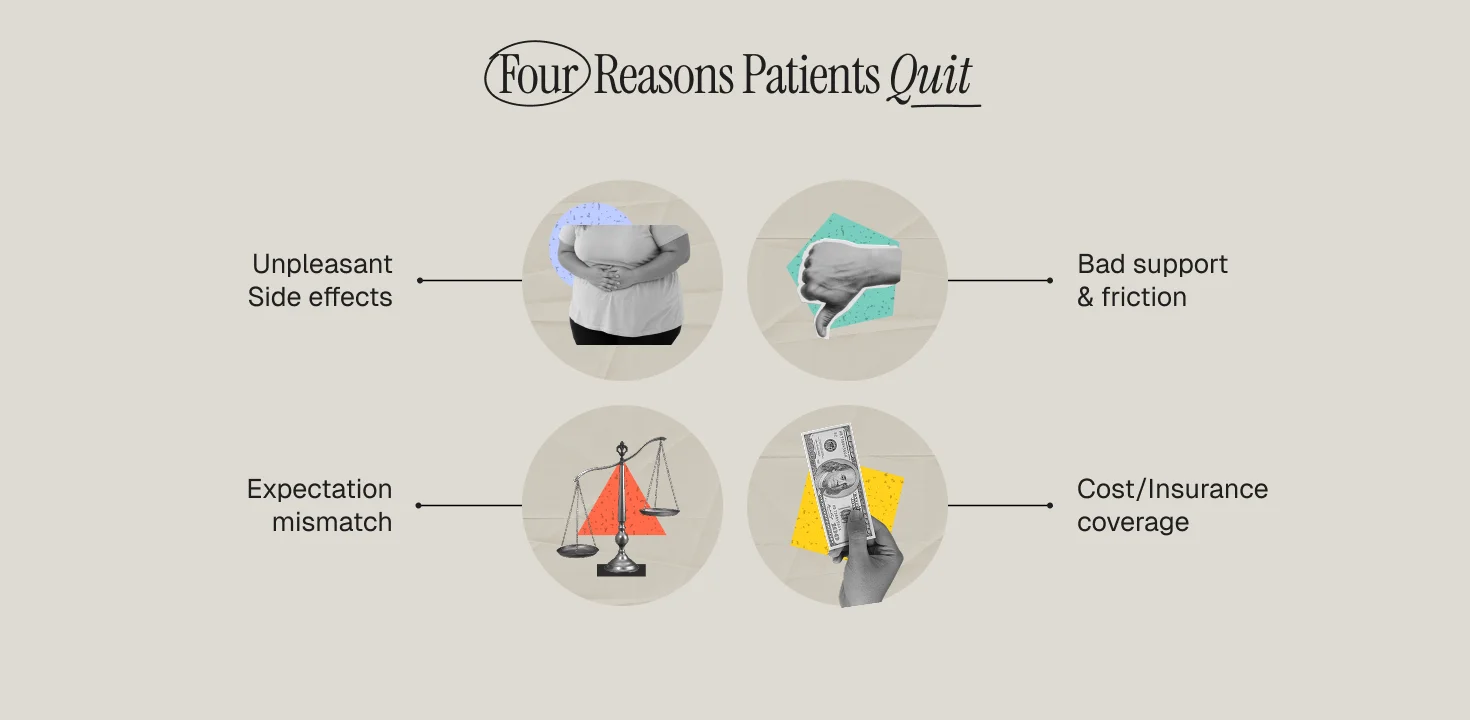
Real-world data and clinical surveys converge on four drivers. First, side effects. Gastrointestinal side effects (nausea, vomiting) are the most common reason patients stop, and they peak early — exactly when patients have the least context to interpret them. Second, cost and coverage. Many patients lose insurance coverage or hit affordability walls; the Blue Health Intelligence brief notes a large share simply stop receiving covered refills. Third, expectation mismatch. Patients who expect fast, linear weight loss quit when week three looks like a plateau. Fourth, friction. Missed refills, clunky check-ins, and slow provider messaging turn a motivated patient into a lapsed one. Notice that three of the four are addressable with lifecycle communication — not with the drug itself.
The First 30 Days Are the Product
If 30% of patients quit in month one, then month one is not onboarding — it is the product experience. A GLP-1 brand that wins retention treats the first 30 days as a designed clinical narrative: what to expect on the titration schedule, how to manage nausea before it happens, when weight change is normal to stall, and how to reach a provider in under an hour. This is the same principle that drives churn reduction through better onboarding in any subscription category, but the stakes are higher here because the alternative to a good first 30 days is a patient who concludes the medicine "didn't work" and tells ten friends.
The operational move is to map every known drop-off trigger to a proactive touch. Injection day one gets a walkthrough. Day three (nausea onset) gets an anticipatory side-effect guide. Day fourteen (the first plateau) gets an expectation-setting message with data on normal trajectories. Each touch is timed to the biology, not to a generic drip calendar. That is what separates regulated telehealth retention from a DTC promo sequence.
The GLP-1 Retention System
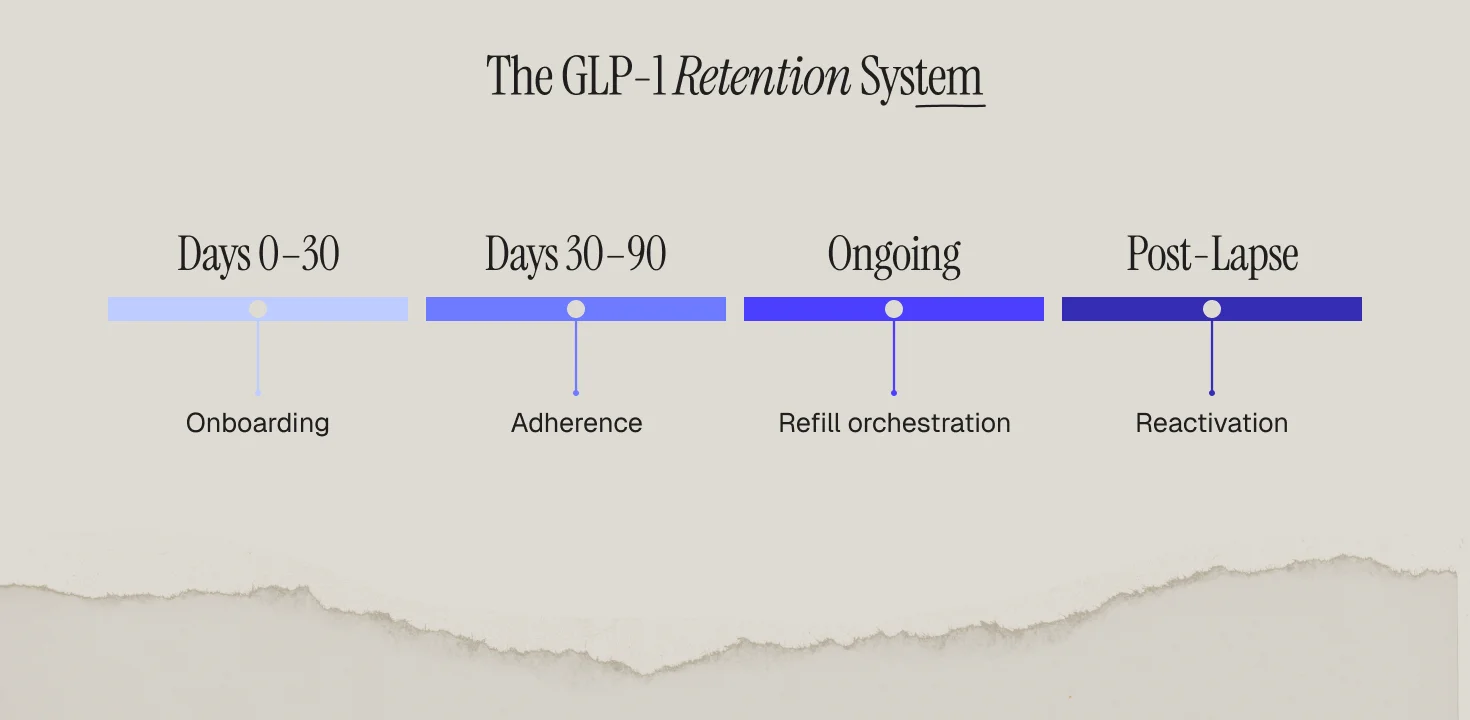
1. Onboarding (Days 0–30): clinical expectation-setting, injection training, side-effect pre-emption, and a fast provider channel. Goal: get the patient to their second dose confidently.
2. Adherence (Days 30–90): titration reminders, symptom check-ins, and progress reframing that counts non-scale wins. Goal: survive the plateau and the titration step-ups. Brands that make it past 90 days see materially better long-run persistence, which is why keeping subscribers beyond 90 days is the pivotal retention milestone.
3. Refill orchestration (ongoing): predictive refill timing so the patient never has a gap between shipments, plus proactive cost/coverage support before the affordability wall hits. A single missed refill is often the first domino of churn.
4. Reactivation (post-lapse): win-back sequences for patients who paused, framed around re-starting safely rather than "we miss you." The online-pharmacy retention playbook covers the compliant mechanics of Rx reactivation.
Metrics That Predict GLP-1 Churn
Stop reporting on aggregate churn after it happens. The leading indicators are: second-dose completion rate (did they get past injection anxiety?), day-14 engagement (did they open the plateau message?), refill-gap days (any gap over zero is a risk flag), and side-effect ticket volume in week one. Each is an early-warning signal you can act on. Building the segmentation to catch these patients before they lapse is exactly the muscle described in how to identify users who are about to churn. The brands that win the GLP-1 decade will not be the ones with the best ad creative — they will be the ones whose lifecycle system quietly keeps patients on therapy long enough to succeed.
Frequently Asked Questions
What is a good GLP-1 patient retention rate?
Benchmarks vary, but given that ~58% discontinue before a meaningful benefit, any program keeping a majority of patients past 90 days is materially outperforming the market. Track persistence by cohort month rather than a single blended number.
Why do so many GLP-1 patients stop in the first month?
Early gastrointestinal side effects, injection anxiety, cost shock, and expectation mismatch all peak in weeks 1–4. Blue Health Intelligence found 30% quit within the first month — the highest-leverage window for lifecycle support.
Is GLP-1 retention different from normal DTC retention?
Yes. The product only delivers value if the patient stays clinically compliant, and communication is regulated. It requires anticipating biology (titration, side effects) and staying HIPAA-aware, unlike a standard DTC retention funnel.
What channels work best for GLP-1 adherence?
A blend: SMS for time-sensitive dose and refill nudges, email for education and expectation-setting, and fast in-app provider messaging for side-effect concerns. Orchestrate them so the patient never gets a gap or a mixed message.
How does refill timing affect retention?
A refill gap is one of the strongest churn predictors. Predictive refill orchestration — shipping before the patient runs out and resolving coverage issues proactively — removes the most common involuntary-churn trigger.


![Featured image: Subscription Retention Strategies: How to Keep Subscribers Beyond 90 Days [2025 Guide]](https://cdn.prod.website-files.com/69bbf9f7f2a3f75341357ebc/69f4b508f4dc60785ebaaf64_69c7cedddc6c12e3e9aeb102_698ae476c97c64c12d4b1033_685e9ef7195ed0904d788146_Retention%25252520That%25252520Converts-2-min.png)
