
Summarize this documentation using AI
Telemedicine marketing is the discipline of acquiring patients for virtual-care services and keeping them engaged through their care journey, using search, paid media, content, email, and retention programs, all inside healthcare's compliance guardrails. It differs from generic healthcare marketing in one decisive way: the entire funnel is digital, so the same channels that acquire a patient also deliver the product. This guide covers the strategies, channels, budget logic, compliance rules, and real-world examples virtual-care brands need in 2026.
Key Takeaways
- The global telehealth market was worth $123.26 billion in 2024 and is projected to reach $455.27 billion by 2030, a 24.68% CAGR, which means patient acquisition costs will keep inflating as competition compounds.
- Demand is mainstream: 37% of US adults used telemedicine in a 12-month period per the CDC's National Health Interview Survey.
- Health is one of the largest search categories on the internet: roughly 7% of Google searches are health-related, about 70,000 per minute, which makes SEO the structural acquisition channel for virtual care.
- Acquisition is only half the model. Telemedicine unit economics are decided in the first 30-90 days of the patient lifecycle, the retention window we map in our telemedicine retention and lifecycle guide.
- Compliance is a marketing capability, not a legal afterthought: HIPAA limits tracking pixels and retargeting, so first-party data and consented email/SMS carry more of the load than in DTC.
What Telemedicine Marketing Is (and Is Not)
Telemedicine marketing covers every touch that moves a person from symptom or intent to a booked virtual visit, and from a first visit to an ongoing care relationship. It is not hospital brand advertising, and it is not classic DTC ecommerce marketing either. The product is regulated, the claims are constrained, the data is protected, and the purchase is high-trust. A telemedicine funnel that copies a supplement brand's playbook — aggressive discounting, pixel-heavy retargeting, urgency copy — tends to trip both regulators and patient trust.
The operating mental model: acquisition channels earn the first visit; the lifecycle program earns every visit after it. Both are marketing's job.
The Market Context in 2026
Three numbers frame every telemedicine marketing plan this year. First, the category is growing fast: $123.26B in 2024, projected to $455.27B by 2030 at 24.68% CAGR. Growth attracts entrants, and entrants bid up CPCs on the same condition keywords. Second, adoption is no longer the barrier: more than a third of US adults (37%) have used telemedicine within a year. The market's question has shifted from "will patients try virtual care?" to "which brand will they trust, and will they stay?" Third, discovery still starts at a search box: about 7% of all Google searches are health-related — roughly 70,000 a minute, over a billion a day. Brands that own condition-level and service-level queries own the cheapest durable demand.
The 6 Core Channels, Compared
Two notes on the table. Paid search on condition terms (weight loss, HRT, mental health) is effective but expensive and policy-constrained; it should fund the SEO moat, not replace it. And email/SMS is the only channel on the list that compounds with zero media spend — the mechanics for virtual-care brands are covered in our telemedicine retention playbook and, for Rx fulfillment models, our online pharmacy lifecycle guide.
Telemedicine Marketing Strategies That Drive Bookings
1. Own the condition query, not just the brand query. Patients search symptoms and treatments, not company names. Build condition hubs (one per service line) with clinically reviewed content, then point service pages at them. This is where telemedicine digital marketing lives or dies, because health queries happen 70,000 times a minute and the winner of each query pays nothing per click.
2. Make the booking path shorter than the anxiety. Every telemedicine funnel loses patients between "interested" and "seen." Async intake forms, transparent pricing on the page, and same-day appointment availability are conversion assets, not ops details. Publish real prices; insurance ambiguity is the largest silent objection in virtual care.
3. Deploy proof at the decision point. Reviews, clinician credentials, and visit counts belong on the booking page, not the About page. Regulated categories cannot promise outcomes, so borrow credibility instead: board certifications, affiliations, security posture, and volume served.
4. Treat email capture as a first-class conversion. Not everyone books on visit one. A consented email or SMS opt-in converts the maybe-later cohort over weeks. The welcome-to-first-visit sequence is the highest-ROI asset in telemedicine marketing services engagements, and it is also the most commonly missing one.
5. Run paid to fill the gaps SEO has not won yet. Paid search on bottom-funnel service terms, paid social for demand creation in look-alike-free, condition-aware contexts (interest and content targeting, not health-data targeting). Expect platform policy reviews; build creative variants that describe the service without diagnosing the viewer.
6. Borrow distribution through partnerships. Employers, payers, pharmacies, and complementary health brands already own patient trust. Co-marketing and referral programs convert at rates paid media cannot touch, at a fraction of the cost.
Retention: The Half of the Funnel Most Brands Skip
Virtual-care brands routinely spend 90% of budget acquiring a patient who lapses after one visit. The correction is a lifecycle program that treats the first 30 days as part of the product: onboarding that sets expectations before the first appointment, adherence and refill nudges timed to the care plan, reactivation triggered by lapsed-visit signals, and win-back for the 90-day silent cohort. For subscription-model care (weight management, HRT, dermatology), the mechanics are identical to the ones we document in our telemedicine retention and lifecycle guide; for brands with an in-house pharmacy leg, see the online pharmacy playbook. The teardown of how the biggest player in the category re-engineered its model around recurring care is in our Hims & Hers GLP-1 retention analysis.
Compliance Guardrails
Three constraint sets shape every campaign. HIPAA: no PHI in ad platforms, analytics pixels configured for consent, marketing communications to patients require authorization when they reference treatment. In practice this pushes telemedicine brands toward first-party data, server-side measurement, and owned channels. FTC: substantiation for any outcome claim, clear disclosure on testimonials, and honest pricing. State telehealth rules: licensure boundaries mean geo-targeting is a compliance function; do not advertise services in states where your clinicians cannot practice. None of this is optional, and all of it is survivable with process: legal review templates for claims, a pre-approved language library, and consent-first data architecture.
Budget and Team: Agency, In-House, or Hybrid
Under roughly $50k/month of total marketing spend, a hybrid usually wins: in-house ownership of brand and clinical review, specialist partners for SEO/content and lifecycle. A telemedicine digital marketing agency or telemedicine marketing company earns its fee when it brings healthcare-specific pattern recognition — compliance-cleared creative, condition-keyword maps, HIPAA-aware martech — rather than generic DTC tactics with a stethoscope logo. For the email/CRM leg specifically, the vendor landscape is mapped in our healthtech email marketing agency comparison. Whatever the structure, keep measurement and the patient database in-house; agencies should operate your accounts, not own your data.
Examples Worth Studying
Hims & Hers rebuilt a transactional telehealth funnel into a recurring-care membership, with weight management as the wedge — the retention mechanics are dissected in our 2026 teardown. Teladoc Health shows the B2B2C route: distribution through employers and payers rather than consumer paid media. Ro is the reference for condition-hub SEO plus vertically integrated pharmacy fulfillment. Talkspace demonstrates category-creation advertising in mental health, and the compliance scars that come with it. Study the pattern, not the logo: every winner pairs one dominant acquisition channel with an unusually disciplined lifecycle program.
How to Measure It
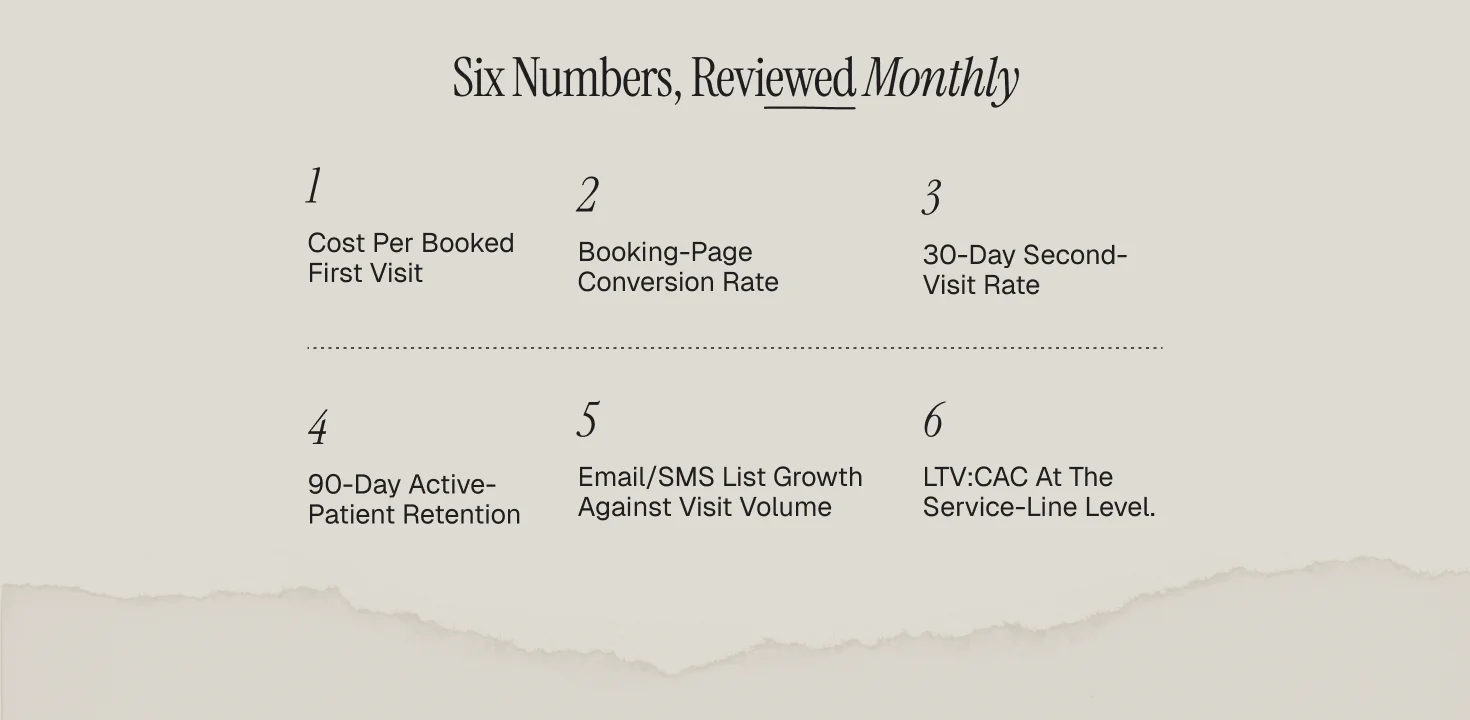
Six numbers, reviewed monthly: cost per booked first visit (by channel), booking-page conversion rate, 30-day second-visit rate, 90-day active-patient retention, email/SMS list growth against visit volume, and LTV:CAC at the service-line level. The 30-day second-visit rate is the single best leading indicator in the set; if it is under 40%, fix onboarding before buying more traffic. Retention math compounds: a brand acquiring 1,000 patients a month at 60% 90-day retention needs 33% less acquisition spend than the same brand at 40% to hold identical active-patient counts.
Frequently Asked Questions
What is telemedicine marketing?
The full set of strategies used to acquire patients for virtual-care services and retain them through the care journey — SEO, paid media, content, partnerships, and lifecycle email/SMS — executed inside HIPAA, FTC, and state telehealth rules.
How big is the telemedicine opportunity?
The global telehealth market was $123.26B in 2024 and is projected to hit $455.27B by 2030 (24.68% CAGR), with 37% of US adults already using telemedicine annually.
What is the most effective telemedicine marketing channel?
SEO for durable acquisition (health queries run ~70,000 per minute on Google) and lifecycle email/SMS for retention. Paid search converts fastest but inflates with competition.
How is telemedicine marketing different from healthcare marketing?
The funnel is fully digital, the service is often subscription-shaped, and the same channels that acquire the patient deliver ongoing care — so retention marketing is a core function, not an afterthought.
Can telemedicine brands use retargeting ads?
Only in narrow, consented configurations. HIPAA guidance treats health-condition inference from tracking as protected, so most brands shift budget to first-party data, contextual targeting, and owned channels.


![Featured image: How HealthTech Apps Can Improve Customer Retention in 2025? [Expert Guide]](https://cdn.prod.website-files.com/69bbf9f7f2a3f75341357ebc/69f4b4952b919dd9bd4f1aa9_69c7cebde8051f4e1dd257e4_698ae4536010effb729a65f9_684e6b4fbf7e32c28a8f0eae_Health%25252520Tech%25252520Retention%25252520(1).png)
