
Summarize this documentation using AI
Telehealth SEO is the practice of ranking a virtual-care service for the condition, treatment, and service queries patients actually type, so the practice acquires patients without paying for every click. It matters because health is one of the internet's largest search categories — about 7% of all Google searches are health-related, roughly 70,000 per minute — and because paid CPCs in telehealth keep inflating as the market grows. Below are the 10 tactics that move rankings for virtual-care practices in 2026, in priority order.
Key Takeaways
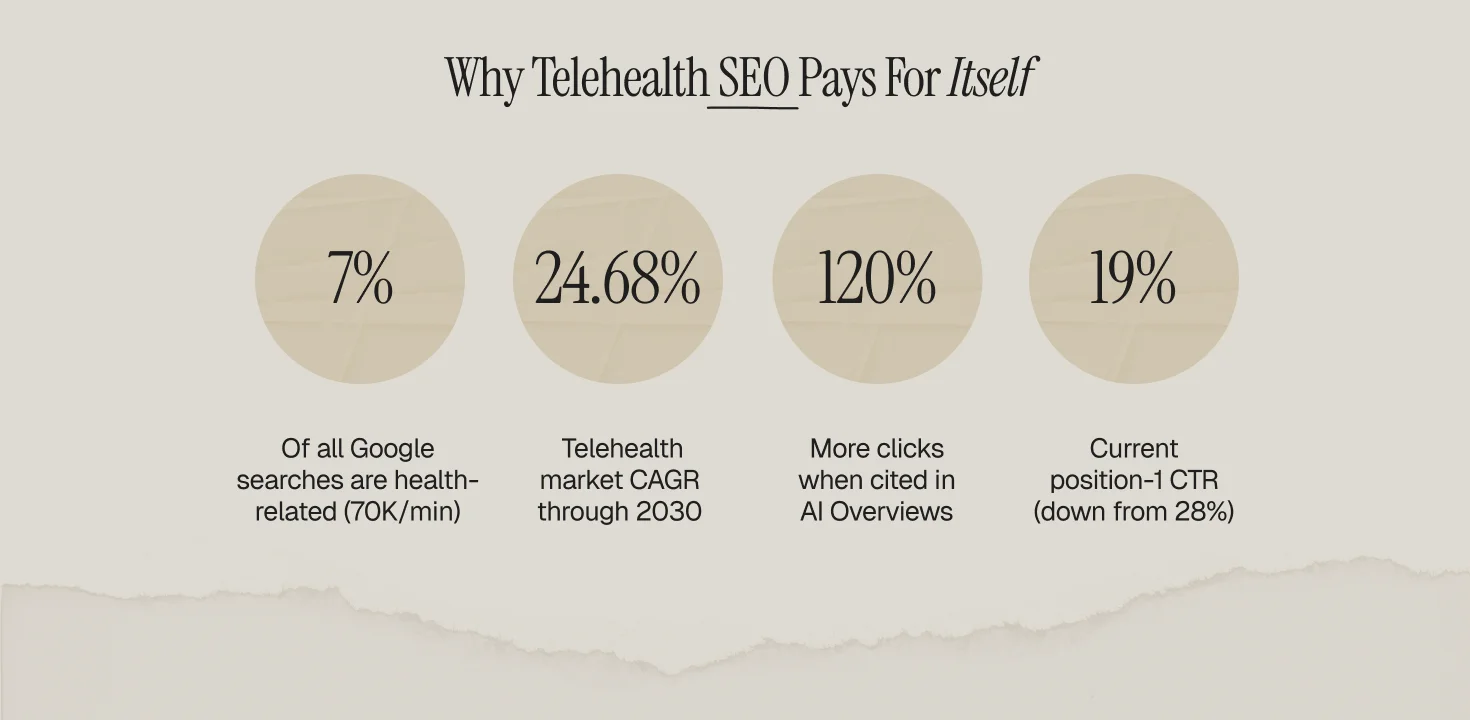
- Health queries run at ~70,000 per minute on Google; owning even narrow condition queries outperforms renting them through ads.
- Organic clicks are getting scarcer: position-1 CTR fell from 28% to 19% year over year as AI Overviews absorb clicks, and pages cited inside AI Overviews earn roughly 120% more clicks per impression than uncited pages — so answer-ready formatting is now a ranking-adjacent skill.
- E-E-A-T is the gatekeeper in health (a YMYL category): clinician review, author credentials, and citations are table stakes, not polish.
- The telehealth market's 24.68% CAGR through 2030 guarantees rising competition; the SEO moat compounds while paid costs inflate.
- Ranking is step one; the visit-to-visit retention system that monetizes the traffic is covered in our telemedicine lifecycle guide.
1. Build Condition-First Site Architecture
Patients search "online treatment for anxiety," not "virtual-care platform." Structure the site as condition hubs (one per service line: weight management, mental health, HRT, dermatology) with treatment and symptom spokes underneath, each internally linked up to its hub. This hub-and-spoke architecture concentrates authority: every spoke that ranks passes relevance to the hub, and the hub ranks for the head term. It is the same structure this article sits inside.
2. Put Clinicians on Every Page (E-E-A-T)
Health is a YMYL (Your Money or Your Life) category, so Google's quality systems weight expertise and trust heavily. Every clinical page needs a named medical reviewer with credentials and a linked bio, a visible review date, and citations to primary sources (journals, CDC, FDA). Pages without clinical review are the first casualties of every core update in this category.
3. Write for the AI Overview, Not Just the SERP
The click math changed: position-1 organic CTR dropped from 28% to 19% as AI Overviews spread, but pages cited inside an AI Overview earn about 120% more clicks per impression than uncited pages on the same query. The tactic: open every page with a 2-3 sentence direct answer, use question-format H2s, keep one claim per sentence, and attach a source to every statistic. You are writing to be quoted.
4. Target Service + State Queries
Licensure makes geography a keyword modifier: "online psychiatrist California," "telehealth suboxone Texas." Build state pages only for states where your clinicians practice, list the covered states on every service page, and mark the pages up so search engines understand availability. This is also a compliance control — ranking in a state you cannot serve creates a bad patient experience and regulatory exposure.
5. Publish Transparent Pricing Pages
"How much does an online doctor visit cost" and its variants carry enormous intent, and most competitors hide the answer behind intake funnels. A real pricing page (visit cost, subscription tiers, insurance handling) ranks for money queries, feeds the AI Overview, and pre-answers the biggest booking objection. Money pages convert best when paired with proof elements: clinician counts, visit volume, security posture.
6. Earn Health-Grade Backlinks
Generic guest posts do little in YMYL. What moves authority: clinician quotes to health journalists, original data (publish your anonymized outcomes or utilization data), partnerships with patient-advocacy organizations, and citations from .edu/.gov and medical association pages. One study covered by a health trade outlet outweighs fifty directory links.
7. Fix Technical Health
Virtual-care sites accumulate technical debt fast: intake funnels behind JavaScript, duplicate state pages, unindexed blog archives. The checklist: sub-2.5s LCP on mobile, MedicalWebPage/FAQPage/Physician schema where each applies, one canonical per condition, an XML sitemap that reflects the hub-spoke tree, and no intake-funnel URLs in the index. Crawl the site quarterly; treat every orphaned clinical page as a bug.
8. Capture the Long Tail with FAQ Content
Every condition hub should carry a 5-8 question FAQ mirroring real patient queries ("can a telehealth doctor prescribe antibiotics," "does insurance cover online therapy"). FAQs win featured snippets, populate FAQPage schema, and give AI Overviews quotable blocks. Mine the questions from search console queries, intake-form free text, and support tickets — not from a keyword tool alone.
9. Localize Where Licensure Allows
Even pure-virtual practices benefit from local signals in states with heavy patient concentration: a Google Business Profile where a physical entity exists, state-specific testimonial pages, and content referencing state insurance and licensure specifics. For multi-state groups, the state page template should vary by regulation, not just by find-and-replace of the state name — thin doorway pages get filtered.
10. Measure by Booked Visits, Not Traffic
Rank tracking is vanity if intake does not move. Wire analytics (consent-first, HIPAA-aware — no PHI in URLs or events) to attribute booked first visits to landing pages, then judge every content investment on cost per booked visit against paid search. And close the loop after the click: SEO fills the top of the funnel, but the 30-and-90-day lifecycle program decides whether a ranked page produces a retained patient or a one-visit statistic. For Rx-fulfillment models, the retention leg is mapped in our online pharmacy playbook; the best-in-category example of pairing organic demand with recurring care is dissected in our Hims & Hers GLP-1 teardown.
Frequently Asked Questions
What is telehealth SEO?
The discipline of ranking a virtual-care practice for condition, treatment, service, and pricing queries so it acquires patients organically — executed inside YMYL quality standards and state licensure boundaries.
How long does telehealth SEO take to work?
Typically 3-9 months for meaningful movement on condition terms, faster on long-tail FAQ queries. The compounding is the point: the 24.68% market CAGR inflates paid CPCs every quarter while owned rankings get cheaper per visit.
Do AI Overviews make telehealth SEO pointless?
No — they redistribute clicks. Position-1 CTR fell from 28% to 19%, but pages cited inside AI Overviews earn ~120% more clicks per impression. Answer-ready formatting captures that citation traffic.
Should we hire a telehealth SEO company or do it in-house?
In-house owns clinical review and data; a telehealth SEO agency earns its fee on healthcare-specific link building, condition-keyword maps, and YMYL content ops. Judge any SEO services for telehealth engagement on cost per booked visit, not rankings delivered.
Does telehealth SEO work for niche practices like addiction clinics?
Yes — often better, because query intent is sharp and competition thinner. SEO for a telehealth addiction clinic leans on state + treatment queries, clinician E-E-A-T, and FAQ capture.


![Featured image: How HealthTech Apps Can Improve Customer Retention in 2025? [Expert Guide]](https://cdn.prod.website-files.com/69bbf9f7f2a3f75341357ebc/69f4b4952b919dd9bd4f1aa9_69c7cebde8051f4e1dd257e4_698ae4536010effb729a65f9_684e6b4fbf7e32c28a8f0eae_Health%25252520Tech%25252520Retention%25252520(1).png)
